
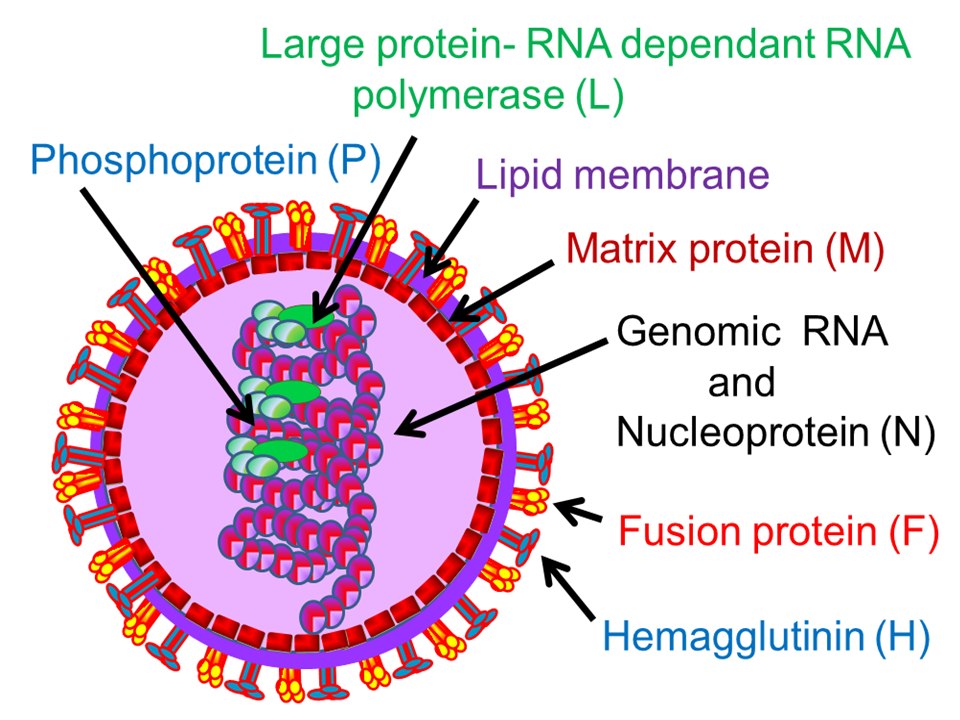
Measles virus (MV) is the causative agent of measles in children. Measles is a highly contagious infectious disease. According to the World Health Organization, about 20 million children worldwide suffer from measles every year. Measles virus is highly contagious and has high morbidity. In addition to causing common cough, high fever, fear of light and rashes all over the face, trunk and upper extremities, it is also easy to be complicated by bronchopneumonia or meningitis, resulting in a high mortality rate. Measles virus belongs to the genus Measles virus of the family Paramyxoviridae. It is spherical and is an enveloped negative-strand RNA virus. The viral genome encodes nucleocapsid protein (N), phosphorylated protein (P/C), matrix protein (M), virulence protein (V), membrane fusion protein (F), hemagglutinin (H) and polymerase (L). Among them, H and F proteins are located on the surface of the viral membrane. During viral infection, H protein binds to host-specific receptor molecules to initiate viral infection of cells. F protein directly mediates the fusion of virus and host cell membrane to complete the virus invasion process. The measles virus receptors that have been discovered so far include CD46 (Membrane cofactor protein, MCP), CD150 (Signaling lymphocyte activation molecule, SLAM) and the recently discovered Nectin-4 (Poliovirusreceptor-related protein 4, PVRL4). The discovery of these receptors has greatly facilitated the study of the release mechanism of measles virus infection.
Measles virus infection process in the past, it was believed that the measles virus infects the host through the upper respiratory tract. However, studies in recent years have shown that alveolar macrophages and DC cells express abundant SLAM molecules on the surface, which are the target cells of the early infection of the measles virus. The synapses of immature DC cells can capture the virus through alveolar epithelial cells, and the process of virus infection of DC cells is roughly through the following mechanism: Although the immature DC cell surface does not express SLAM, measles virus and DC-cell surface DC- SIGN interacts to induce the activation of neutral and acidic sphingomyelinase (SMase), and DC-SIGN-dependent SMase activation recruits SLAM from the intracellular reservoir to the cell surface, promoting viral infection. Infected DC cells carry the virus into the draining lymph nodes and present the virus to monocytes, T cells, and B cells. The virus replicates in these infected lymphocytes, causing initial viremia. The amplified virus further infects secondary lymphoid organs such as thymus, spleen, tonsils, etc., resulting in secondary viremia and acute immunosuppression. The virus then spreads further, infects the skin, kidneys, gastrointestinal tract, liver, and respiratory tract through Nectin-4 receptors expressed on the surface of epithelial cells, replicates in large numbers in epithelial cells, and is then released from the top of the epithelial cells by coughing or sneeze is transmitted to another individual.
Measles Virus Specific Antibody Test
After measles virus infection, specific antibodies are detected for the specific immune response produced by the human body. All specimens containing measles virus antibodies, such as blood, serum, mouthwash, body fluids, etc., can be used as objects for antibody detection. Measles virus can be detected in a throat swab or blood sample a few days before or 3 days after a measles attack. Three to five days after the onset of the rash, the positive rate of virus detection in the samples gradually decreased. The commonly used methods for measles virus antibody detection currently mainly include Enzyme-linked immunosorbent assay (ELISA), Hemagglutination inhibition test (HI), Plaque reduction neutralization test (Plaque reduction neutralization test, PRNT) and complement fixation test (CFT), etc., can be used for the diagnosis of suspected measles patients, the evaluation of the immune status of the population, and the epidemiological investigation.